

Kawasaki Disease



Categories
Recent News - Kawasaki Disease Foundation India
SUMMARY OF NEWER THERAPEUTIC STRATEGIES (2012 IKDS)
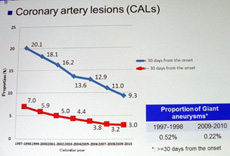
IVIG RESISTANT KD OFTEN DEVEOPE CORONARY ARTERY LESIONS (CAL)
IVIG RESISTANT KD OFTEN DEVEOPE CORONARY ARTERY LESIONS (CAL)
Optimal regimen for managing KD AND unresponsive to IVIG therapy is still unclear
Study from Tokyo metropolitan Children’s Medical centre
1. Steroid pulse therapy to unresponsive IVIG therapy
IVIG RESISTANCE to initial IVIG dose 15-20% . Additional IVIG shows 71% response 30% resistance. 100 % responded to additional IVMP alone
IVIG + Aspirin within 10days of onset
If unresponsive second dose of IVIG 2g/kg/bwt to be given. Further not responsive to second dose IVIG, give IVMP (Methyl Prednisolone pulse therapy) 30mg/kg/day x 3days followed by oral 2-4 wk
2. Primary corticosteroid therapy to standard IVIG regimen may improve CAL in severe KD (Risk score >5) trial in 121 patients each with MP +IVIG +Asprin and IVIG –Aspirin alone showed 3% vs 23% response.
3. Infliximab, human monoclonal Ab thats binds specifically to TNF a (proinflammatory cytokines) 5mg/kg BWT infusion for recrudescent fever or IVIG resistant cases.
4. CYCLOSPORIN - A Hiroyuki Susuki Wakayama Medical University
ITPKC (INOSITOL TRIPHOSHATE 3-KINASE C) act as anegative regulator of T cell activation and activated T cells may play a pivotal role in pathogenesis of KD. Hence Cyclosporin-A will suppresses the activity of T cell. Dose 4-8mg/Kg/Day PO x 5-6 days depends on a febrile period.
5. METHOTREXATE is a folic acid antagonist suppresses lymphocyte proliferation and has role in modulatingcytokines especially IL-6 highly expressed in KD.
6. ULINASTATIN Takahiro - National defence Medical college
in patient with KD markedly activated neutrophils or high plasma neutrophil elastase have been implicated in poor response to IVIG AND CAL.
Treated with ULST as Initial treatment to KD , occurrence of Cal was significantly lower 3% than 7% in control group.
7. Antioxidants +ASA+IVIG
8. Many studies found that initial treatment with 1 gram IVG is similar results with 2 gm IVIG. This will rethink our treatment strategies in developing countries like us
9. There is no role in giving high dose Aspirin as per many studies even 30mg/kg/BWT is still effective when we think about adverse events to ASA. But many do not want to take risk and may give 60-80mg/kg/bwt Q6H
10. Kawaski patient rarely present with hypotension so called Kawasaki shock syndrome . Hponatremia is a presenting symptom. Hnece checking electrolyte during acute pahse is justifiable
11. Rarely pappilary edema can develop . Hnece Fundus exam also necessary to r/o papilledema.
12. Asymptomatic pyuria may associated with severe coronary artery lesion. Hence urinary PC cases we should be careful in treating CAL
13. Plasma exchange may be the final choice for refractory KD
IVIG RESISTANCE to initial IVIG dose 15-20% . Additional IVIG shows 71% response 30% resistance. 100 % responded to additional IVMP alone
IVIG + Aspirin within 10days of onset
If unresponsive second dose of IVIG 2g/kg/bwt to be given. Further not responsive to second dose IVIG, give IVMP (Methyl Prednisolone pulse therapy) 30mg/kg/day x 3days followed by oral 2-4 wk
2. Primary corticosteroid therapy to standard IVIG regimen may improve CAL in severe KD (Risk score >5) trial in 121 patients each with MP +IVIG +Asprin and IVIG –Aspirin alone showed 3% vs 23% response.
3. Infliximab, human monoclonal Ab thats binds specifically to TNF a (proinflammatory cytokines) 5mg/kg BWT infusion for recrudescent fever or IVIG resistant cases.
4. CYCLOSPORIN - A Hiroyuki Susuki Wakayama Medical University
ITPKC (INOSITOL TRIPHOSHATE 3-KINASE C) act as anegative regulator of T cell activation and activated T cells may play a pivotal role in pathogenesis of KD. Hence Cyclosporin-A will suppresses the activity of T cell. Dose 4-8mg/Kg/Day PO x 5-6 days depends on a febrile period.
5. METHOTREXATE is a folic acid antagonist suppresses lymphocyte proliferation and has role in modulatingcytokines especially IL-6 highly expressed in KD.
6. ULINASTATIN Takahiro - National defence Medical college
in patient with KD markedly activated neutrophils or high plasma neutrophil elastase have been implicated in poor response to IVIG AND CAL.
Treated with ULST as Initial treatment to KD , occurrence of Cal was significantly lower 3% than 7% in control group.
7. Antioxidants +ASA+IVIG
8. Many studies found that initial treatment with 1 gram IVG is similar results with 2 gm IVIG. This will rethink our treatment strategies in developing countries like us
9. There is no role in giving high dose Aspirin as per many studies even 30mg/kg/BWT is still effective when we think about adverse events to ASA. But many do not want to take risk and may give 60-80mg/kg/bwt Q6H
10. Kawaski patient rarely present with hypotension so called Kawasaki shock syndrome . Hponatremia is a presenting symptom. Hnece checking electrolyte during acute pahse is justifiable
11. Rarely pappilary edema can develop . Hnece Fundus exam also necessary to r/o papilledema.
12. Asymptomatic pyuria may associated with severe coronary artery lesion. Hence urinary PC cases we should be careful in treating CAL
13. Plasma exchange may be the final choice for refractory KD
INCIDENCE of KD Coronary
Artery Disease in JAPAN
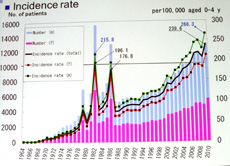
Incidents of KD in Japan 2012
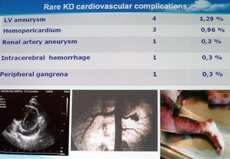
Rare Complications