

Kawasaki Disease



Categories
What is Kawasaki Disease ?
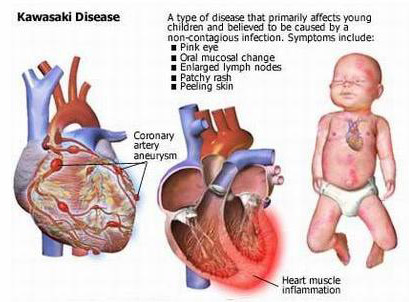
Kawasaki disease (KD), also known as caca syndrome, crap syndrome and Mucocutaneous lymph node syndrome is an autoimmune disease that manifests as a systemic necrotizing medium-sized vessel vasculitis and is largely seen in children under 5 years of age. It affects many organ systems, mainly those including the blood vessels, skin, mucous membranes and lymph nodes; however, its most serious effect is on the heart where it can cause severe coronary artery aneurysms in untreated children. Without treatment, mortality may approach 1%, usually within 6 weeks of onset. With treatment, the mortality rate is less than 0.01% in the U.S.
 There is often a pre-existing viral infection that may play a role in its pathogenesis. The conjunctival and oral mucosa, along with the epidermis (skin), become erythematous (red and inflamed). Edema is often seen in the hands and feet and the cervical lymph nodes are often enlarged. Also, a remittant fever, often 40℃ (104°F) or higher, is characteristic of the acute phase of the disease. In untreated children, the febrile period lasts on average approximately ten days, but may range from 5 to 25 days. The disorder was first described in 1967 by Dr. Tomisaku Kawasaki in Japan.
There is often a pre-existing viral infection that may play a role in its pathogenesis. The conjunctival and oral mucosa, along with the epidermis (skin), become erythematous (red and inflamed). Edema is often seen in the hands and feet and the cervical lymph nodes are often enlarged. Also, a remittant fever, often 40℃ (104°F) or higher, is characteristic of the acute phase of the disease. In untreated children, the febrile period lasts on average approximately ten days, but may range from 5 to 25 days. The disorder was first described in 1967 by Dr. Tomisaku Kawasaki in Japan.
 Classification
Classification
Proliferation, as well as the specific type of tissue damage occurring within the vein or arterial walls. Under this to be a necrotizing vasculitis (also called necrotizing angeititis), which may be identified histologically by the occurrence of necrosis (tissue death), fibrosis, and proliferation of cells associated with inflammation in the inner layer of the vascular wall.[6][7] Other diseases featuring necrotizing vasculitis include Polyarteritis nodosa, Wegener's granulomatosis, Henoch-Schönlein purpura and Churg-Strauss syndrome. Kawasaki disease may be further classified as a medium-sized-vessel vasculitis, affecting medium and small sized blood vessels, such as the smaller cutaneous vasculature (veins and arteries in the skin) that range from 50 to 100µm in diameter. KD is also considered to be a primary childhood vasculitis, a disorder associated with vasculitis that mainly affects children under the age of 18. A recent, consensus-based evaluation of vasculitides occurring primarily in children resulted in a classification scheme for these disorders, to both distinguish them and suggest a more concrete set of diagnostic criteria for each. Within this classification of childhood vasculitides, Kawasaki disease is, again, a predominantly medium-sized vessel vasculitis. It is also an autoimmune form of vasculitis, and is not associated with ANCA antibodies, unlike other vasculitic disorders associated with them, such as wegener's granulomatosis, microscopic polyangiitis, and Churg-Strauss syndrome. This categorization is considered essential for appropriate treatment
There is often a pre-existing viral infection that may play a role in its pathogenesis. The conjunctival and oral mucosa, along with the epidermis (skin), become erythematous (red and inflamed). Edema is often seen in the hands and feet and the cervical lymph nodes are often enlarged. Also, a remittant fever, often 40℃ (104°F) or higher, is characteristic of the acute phase of the disease. In untreated children, the febrile period lasts on average approximately ten days, but may range from 5 to 25 days. The disorder was first described in 1967 by Dr. Tomisaku Kawasaki in Japan.Proliferation, as well as the specific type of tissue damage occurring within the vein or arterial walls. Under this to be a necrotizing vasculitis (also called necrotizing angeititis), which may be identified histologically by the occurrence of necrosis (tissue death), fibrosis, and proliferation of cells associated with inflammation in the inner layer of the vascular wall.[6][7] Other diseases featuring necrotizing vasculitis include Polyarteritis nodosa, Wegener's granulomatosis, Henoch-Schönlein purpura and Churg-Strauss syndrome. Kawasaki disease may be further classified as a medium-sized-vessel vasculitis, affecting medium and small sized blood vessels, such as the smaller cutaneous vasculature (veins and arteries in the skin) that range from 50 to 100µm in diameter. KD is also considered to be a primary childhood vasculitis, a disorder associated with vasculitis that mainly affects children under the age of 18. A recent, consensus-based evaluation of vasculitides occurring primarily in children resulted in a classification scheme for these disorders, to both distinguish them and suggest a more concrete set of diagnostic criteria for each. Within this classification of childhood vasculitides, Kawasaki disease is, again, a predominantly medium-sized vessel vasculitis. It is also an autoimmune form of vasculitis, and is not associated with ANCA antibodies, unlike other vasculitic disorders associated with them, such as wegener's granulomatosis, microscopic polyangiitis, and Churg-Strauss syndrome. This categorization is considered essential for appropriate treatment